
Wrist joint
Brief anatomy and function of wrist joint
-
Wrist joint is NOT a single joint but forms by combinations of many bones and joints
- Distal radio-ulnar joint (DRUJ)
- Radiocarpal
- Ulnocarpal
- Intercarpal
Various bones take part in formation of wrist joint are
- Distal end of radius and Ulna
- 8 Carpal bones
- Proximal end of all 5 metacarpals
- Radiocarpal, ulnocarpal and various intercarpal ligaments bind all these bones together to provide stability
- Proximal Volar aspect of wrist has Flexor retinaculum & dorsal side has dorsal extensor retinaculum
-
Ulnar side of the wrist has TFCC ligament (triangular fibrocartilage complex) comprising of
- Triangular fibrocartilage disc
- Radioulnar ligaments
- Ulnocarpal ligaments
TFCC helps in
- load transmission across the wrist
- Rotation of wrist by stabilizing DRUJ
|
Structures under flexor retinaculum (9 tendon, 1 nerve)
|
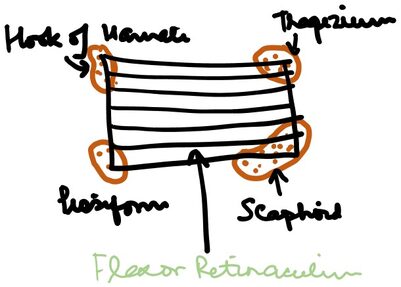
Figure: Anatomy of FR attachment
- Ulnar nerve passes above the Flexor retinaculum via ‘Guyon’s canal’
- The Palmaris longus tendon merges with the flexor retinaculum
- Movements at the wrist joint
|
Movement |
Muscle involved |
|
Palmer Flexion |
FCR, FCU |
|
Dorsiflexion |
ECR, ECU |
|
Radial deviation |
FCR, ECR |
|
Ulnar deviation |
FCU, ECU |
Table showing the movements of the wrist joint and the muscles primarily responsible for the action. FCR, flexor carpi radialis; ECR, extensor carpi radialis; FCU, flexor carpi ulnaris; ECU, Extensor carpi ulnaris
Chief complaints
The patients with wrist pathology mostly come up with specific complaints.
- Pain
- Swelling
- Difficulty in movement
- Subluxation or dislocation
1. Pain: Most common complaint
-
Insidious/acute in onset.
- Acute pain: trauma, acute infection
- Insidious: arthritis, chronic infection, tumors
- Infections and tumors may cause night pain
- Night pain is also seen in carpal tunnel syndrome radiating to the thumb and other 2 ½ lateral fingers
2. Difficulty in movements: Any difficulty in movement at the wrist joint could be due to following common reasons:
- Pain: arising out of any pathology
- Stiffness: post traumatic, RSD
- Arthritis
- Nerve palsy
3. Swelling: Both localized/diffuse swelling is common
- Localized: ganglion
-
Diffuse:
- Traumatic injury
- Infection: Tuberculosis
- Inflammatory: Rheumatoid, cellulitis Synovitis of wrist (due to rheumatoid)
- Tumors
- Others: Reflex sympathetic dystrophy
4. Deformity: it could be due to
- Traumatic: Malunited colles # leads to Manus valgus deformity
- Infections: Tuberculosis
- Rheumatoid: Manus valgus
General & systemic examination: As per standard norms
e.g.: General & systemic examination is relevant in case of rheumatoid arthritis
Local examination
- Attitude: Wrist examination is performed in sitting. The attitude of the wrist and hand can be described.
- Inspection:
Inspect the hand from volar and dorsal aspect
General findings
- Scar: carpal tunnel release scar
- Sinus
- Nail changes
Specifics to look for
- Deformity of wrist: Manus valgus
- Deformity in fingers: especially in Rheumatoid arthritis
- Nail changes: Psoriatic arthritis
- Swelling in hand and fingers
- Muscle wasting of hand and forearm: especially in never injuries (thenar, hypothenar and interossei)
- Bouchard and Heberden Nodes at PIP and DIP in case of osteoarthritis of hand
-
Palpation
- Local rise in temperature
- Tenderness: always palpate in a sequence to look for tender spots in following area. It is better to start on dorso-radial side of snuffbox and proceed in a circular fashion ulnar wards and come back to the original point
- Distal end of radius (volar and dorsal)
- Tip of radial styloid process and 1” proximal area for tenderness over the tendons of APL and EPB
- Anatomical snuff box: look for Scaphoid tenderness
- DRUJ
- Dorsal carpals especially lunate
- Distal end of ulna
- Tip of ulnar styloid process
- Volar aspect of wrist: for median and ulnar nerve, pisiform
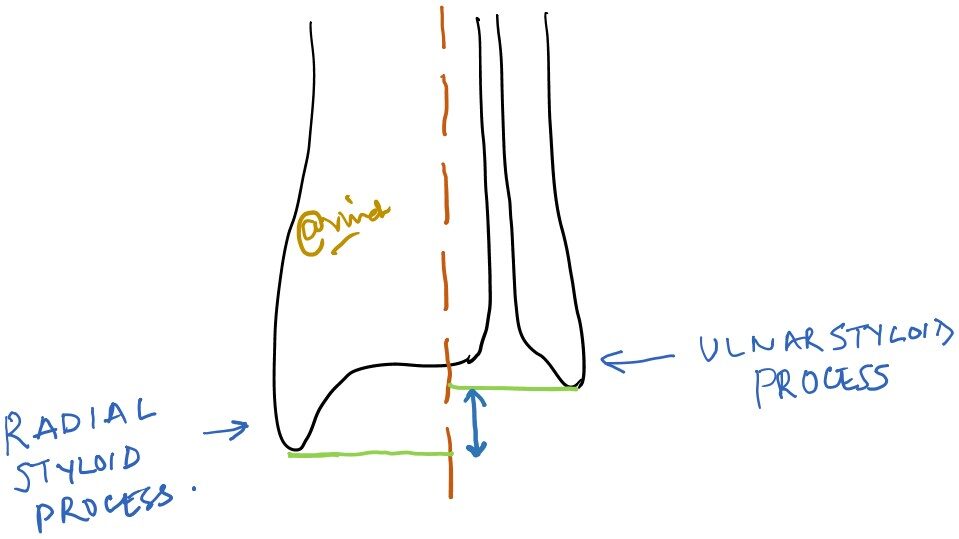
- Two-point relationship- A very important landmark to be palpated is the distance between the tip of two styloid process (radial and ulnar). The radial styloid tip is about 8-14 mm distal to the ulnar styloid tip.
Any disturbance in this relationship is an indicator of deformed distal radius /malunited distal radius.
- Movements: First, one must ask patient to do the active ROM followed by passive ROM of wrist
- Dorsi-flexion
- Palmar-flexion
- Radial deviation
- Ulnar deviation
- Also note the ROM at the various joints f the hand (metacarpophalyngeal and nterphalyngeal)
|
Normal ROM at the wrist Dorsiflexion: 0-700 Palmarflexion: 0-900 Radial deviation: 0-200 Ulnar deviation: 0-40 |
5. Measurments:
- Measurement of the length of upper extremity:
From anterolateral tip of acromion to lateral epicondyle: arm length
From lateral epicondyle to tip of radial styloid process: forearm length
b. The distance between the two styloid process
First a line is drawn over the forearm which represents its midline axis extending from mid-forearm to the wrist joint (brown line). Then a perpendicular is dropped from two styloid process (green). The distance between the two perpendiculars represents the distance between the two styloid process (deep blue).
6. Neurovascular examination of upper limb
7. Joint above: Elbow
8. Special test:
-
For dislocation/subluxation of DRUJ
- Piano key test: Ballottement of the ulna. The distal end of radius is held between thumb and index finger of one hand and distal end of ulna is held between thumb and index by other hand. The Ulna is subjected to ballottement up and down and compared with normal side. An abnormal volar-dorsal movement indicates unstable DRUJ
-
For Carpal Tunnel syndrome (CTS):
- Phalen’s Sign: Patient is asked to completely palmar flex both his wrist by opposing dorsum of both hands against each other. Development of tingling and or numbness in the distribution of median nerve area is indicative of CTS
- Reverse Phalen’s Sign: Patient is asked to completely dorsiflex both his wrist by opposing palm of both hands against each other. Development of tingling and or numbness in the distribution of median nerve area is indicative of CTS
- Durcan’s test: The median nerve under the flexor retinaculum is compressed with the thumb of examiner for 30 seconds. Any tingling and numbness in the area of median nerve is taken as positive Durcan test.
-
For triangular fibrocartilage complex (TFCC) injury:
- Ulnar deviation forearm pronation test: Examiner holds the patients right hand with his right hand and forearm by left hand. Then, the forearm is pronated and wrist is ulnar deviated. This elicits the pain over ulnar aspect of wrist if TFCC is injured.
- Tenderness present over the dorsoulnar aspect of wrist just below the ulnar styloid process.
-
For DeQuervain’s tenosynovitis (Texting thumb/blackberry thumb)
- Finkelstein test: The patient’s affected thumb is grasped and the hand is sharply deviated ulnarwards towards the palm. This elicits tenderness over the anatomical snuff box and area over the radial styloid process in case of De Quervain’s tenosynovitis.
- For 1st carpometacarpal joint arthritis: The patient’s thumb is held by examiner’s hand and then axial stress is given along with rotatory movement of thumb. Pain during such maneuver is indicative of CMC arthritis.
Common conditions affecting wrist with salient features
-
Ganglion
- Affects young patients but can happen in any age
- More common in females
- Presents with: swelling on the dorsum of hand and sometimes on volar aspect usually of pea-size which gives a very firm or bony hard feeling on palpation. Often, size shows variation with time.
- Pathologically: NOT a TRUE CYST. Many theories; synovial herniation/mucus cyst formation/degeneration of connective tissue and cyst formation
- Clinically: Swelling with firm or bony hard felling on palpation
- Diagnosis: MRI/USG
- Treatment: a) Conservative: observation/aspiration and intracystic steroid injection
- b) Surgical excision if painful, large or recurrence after aspiration
-
De Quervain’s Tenosynovitis
- Affects middle age
- Presents with: Pain and swelling along radial border of wrist over the distal end off radius and /anatomical snuff box
-
Pathologically: Tenosynovitis of Abductor Pollicis longus and Extensor Pollicis brevis
- Clinically: Tenderness present over the radial border of wrist and Finkelstein test +
- Diagnosis: MRI/USG
- Treatment:
a) Conservative: NSAIDs, physiotherapy, local steroid injection, thumb splint
b) Surgical release of tendons if conservative treatment fails
-
Mal-united Colles’ fracture
- H/O fall on outstretched hand
- Presents with: Deformity and/pain
- Most common in elderly females and males. Associated osteoporosis
- Pathologically: Malunited distal radius fracture
- Clinically: Manus valgus, the radial and ulnar styloid process are at same level or radial moves proximally.
- Diagnosis: xray
- Treatment:
a) Conservative: NSAIDs, physiotherapy
b) Rarely corrective osteotomy to correct deformity and functional disability.
-
Reflex sympathetic dystrophy (Sudeck’s osteodystrophy)
- Affects any age
- Also known as complex regional pain syndrome (CRPS)
- Mostly after trauma to the wrist and hand. Sometimes even shoulder becomes painful leading to shoulder hand syndrome
- Presents with: Pain, difficulty in moving fingers, swelling of hand and wrist, discoloration of fingers, nails changes, cold hand
- Pathologically: idiopathic dysfunction of sympathetic nervous system of the upper limb after the trauma
-
Clinically:
- Gross swelling of the hand and wrist
- Loss of active and passive movements
- Finger discoloration
- Nail changes
-
Diagnosis: Mostly clinical.
- X-ray of affected part: patchy osteoporosis
- Bone scan: Increased uptake
-
Treatment: ALWAYS conservative; pain relief and physiotherapy is the essence!
- Pain control: NSAIDs
- Pregabalin, carbamazepine
- Vitamin C
- Physiotherapy: gentle active mobilization of affected part
- Limb elevation and compression bandage for edema control
- Local Sympathetic ganglion block to improve pain